Ovulation Disorders – When Eggs are the cause of infertility
Part one: Ovulation disorders and how they are diagnosed.
Ovulation Disorders account for 25% of the main causes of infertility and are usually caused by hormonal issues. Ovulation disorders involve the development of eggs, the release of eggs or the timing of eggs development and release. Ovulations disorders typically result in infrequent or irregular periods or periods without ovulation. The effects of ovulation disorders on fertility are: fewer opportunities to conceive, difficulty detecting a woman’s fertile periods, eggs not breaking through the follicle in order to be fertilized. Also developed eggs might be releasing off sync with a woman’s cycle causing the other factors crucial to fertilization or implantation not to be present.
 Ovulation disorders are usually caused by hormonal issues which are controlled and released by the Endocrine system. Dr. Pinto and Dr. Orkun Tan are specially trained in Reproductive Endocrinology; and are highly educated and experienced in diagnosing and treating these disorders.
Ovulation disorders are usually caused by hormonal issues which are controlled and released by the Endocrine system. Dr. Pinto and Dr. Orkun Tan are specially trained in Reproductive Endocrinology; and are highly educated and experienced in diagnosing and treating these disorders.
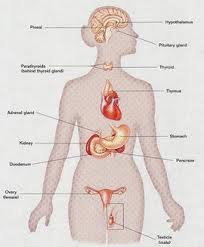
The Female endocrine system is comprised of the Pineal Gland, the Pituitary Gland, the thyroid and parathyroid glands, the Thymus gland, the Adrenal Glands, the Pancreas and the Ovaries. These glands and organs control the release of hormones that are vital for fertility and reproductive health.
Typical Causes of Ovulation Disorders (disrupting or affecting fertility) are:
- Hypothalamus Dysfunction – affects most of the hormones influencing egg development and menstruation.
- Polycystic Ovarian Syndrome– causes issues with ovulation and irregular menstruation (Find out about PCOS Treatment Click Here)
- Luteal Phase Effect – effects endometrial development causing the egg not to implant to the uterus.
- Tumors of the pituitary or adrenal glands or ovaries – affects glands release of hormones that control reproductive health.
- Primary Ovarian Failure – when the ovaries don’t produce normal amounts of the hormone estrogen or release eggs regularly.
- Resistant ovary syndrome – the ovaries are resistant to the hormone releases by your pituitary gland and, as a result, your fertility and menstrual cycles may be irregular.
- Autoimmune oophoritis – is an autoimmune inflammation of ovaries resulting in their destruction, atrophy, and fibrosis with a loss of fertility and ovary hormonal production.
| Female Hormone Levels Guide | ||
| Hormone to Test | Normal | What Value Means |
| 3-20 mIU/ml | FSH is often used as a gauge of ovarian reserve. In general, under 6 is excellent, 6-9 is good, 9-10 fair, 10-13 diminished reserve, 13+ very hard to stimulate. In PCOS testing, the LH:FSH ratio may be used in the diagnosis. The ratio is usually close to 1:1, but if the LH is higher, it is one possible indication of PCOS. | |
| Estradiol (E2) | 25-75 pg/ml | Levels on the lower end tend to be better for stimulating. Abnormally high levels on day 3 may indicate existence of a functional cyst or diminished ovarian reserve. |
| Estradiol (E2) | 100+ pg/ml or 2x Day 3 | There are no charts showing E2 levels during stimulation since there is a wide variation depending on how many follicles are being produced and their size. Most doctors will consider any increase in E2 a positive sign, but others use a formula of either 100 pg/ml after 4 days of stims, or a doubling in E2 from the level taken on cycle day 3. |
| Estradiol (E2) | 200 + pg/ml | The levels should be 200-600 per mature (18 mm) follicle. These levels are sometimes lower in overweight women. |
| Luteinizing Hormone (LH) | < 7 mIU/ml | A normal LH level is similar to FSH. An LH that is higher than FSH is one indication of PCOS. |
| Luteinizing Hormone (LH) | > 20 mIU/ml | The LH surge leads to ovulation within 48 hours. |
| Prolactin | < 24 ng/ml | Increased prolactin levels can interfere with ovulation. They may also indicate further testing (MRI) should be done to check for a pituitary tumor. Some women with PCOS also have hyperprolactinemia. |
| Progesterone (P4) | < 1.5 ng/ml | Often called the follicular phase level. An elevated level may indicate a lower pregnancy rate. If low progesterone levels are an issue for you, consider taking a natural fertility supplement like FertilAid for Women. |
| Progesterone (P4) | > 15 ng/ml | A progesterone test is done to confirm ovulation. When a follicle releases its egg, it becomes what is called a corpus luteum and produces progesterone. A level over 5 probably indicates some form of ovulation, but most doctors want to see a level over 10 on a natural cycle, and a level over 15 on a medicated cycle. There is no mid-luteal level that predicts pregnancy. Some say the test may be more accurate if done first thing in the morning after fasting. |
| Thyroid Stimulating Hormone (TSH) | .4-4 uIU/ml | Mid-range normal in most labs is about 1.7. A high level of TSH combined with a low or normal T4 level generally indicates hypothyroidism, which can have an effect on fertility. |
| Free Triiodothyronine (T3) | 1.4-4.4 pg/ml | Sometimes the diseased thyroid gland will start producing very high levels of T3 but still produce normal levels of T4. Therefore measurement of both hormones provides an even more accurate evaluation of thyroid function. |
| Free Thyroxine (T4) | .8-2 ng/dl | A low level may indicate a diseased thyroid gland or may indicate a non- functioning pituitary gland which is not stimulating the thyroid to produce T4. If the T4 is low and the TSH is normal, that is more likely to indicate a problem with the pituitary. |
| Total Testosterone | 6-86 ng/dl | Testosterone is secreted from the adrenal gland and the ovaries. Most would consider a level above 50 to be somewhat elevated. |
| Androstenedione | .7-3.1 ng/ml | |
| Sex Hormone Binding Globulin (SHBG) | 18-114 nmol/l | Increased androgen production often leads to lower SHBG |
| 17 Hydroxyprogesterone | 20-100 ng/dl | Mid-cycle peak would be 100-250 ng/dl, luteal phase 100-500 ng/dl |
| (Anit-Mullerian Hormone) AMH | Anti-Mullerian Hormone (AMH) is a hormone produced by the cells that support the dormant pool of eggs in the ovaries. Therefore, a higher level of AMH suggests a larger pool of eggs (or a greater ovarian reserve). | |